


5G, Graphene, Covid and Monkeypox Symptoms
Another Virus Fraud

THE PHEIC
The WHO called out another PHEIC (pronounce: FAKE), a Public Health Emergency of International Concern regarding Monkeypox. I set out to see if EMF such as 5G could explain Monkeypox symptoms or if there are other explanations for them that have nothing to do with a virus as a virus was never isolated. First, I looked at what Dr. Andrew Kaufman MD and Dr. Tom Cowan MD have discovered. Then I combed through many studies regarding Covid symptoms as consequence of 5G, the role of Graphene Oxide in combination with EMF/5G as well as other skin diseases that can be sold as Monkeypox.
Dr. Andrew Kaufman MD did a video1 showing that the virus purported to cause Monkeypox has never been isolated. The first paper he discusses is about monkeys in captivity who had puss filled pustules on the skin. They took the puss and put it into cell cultures and observed a cytopathic effect which many know now will happen to cell cultures just be starving and poisoning them with toxic antibiotics. They also injected the puss into the brain and skin of lab animals who then developed symptoms that were unlike the symptoms of the sick monkeys. Electron microscopy showed white squares they interpreted as the virus though the method they used would preclude any material to be on this part of the slide and the photo contrasts the photo shown by the CDC how the purported virus looks like. The CDC photo’s origin is unknown as the CDC doesn’t mention it. He then looks at a few other papers all claiming isolation of the Monkeypox virus, which was not truly isolation of anything just like in all the other virus studies.
Dr. Tom Cowan MD as well did a podcast2 combing through so-called isolation studies. They use the same method of monkey kidney cell cultures, starved and poisoned and observing a cytopathic effect. He further presents an answer by the CDC to a FOIA request that basically states that the CDC does not have records on single virion sequencing that ensured the virion was physically isolated from any other genetic material before sequencing and that they do not have methods to purify a single virion away from all other materials, see photo of the FOIA response below (from Dr. Tom Cowan’s podcast):

Image courtesy of Dr. Tom Cowan MD
Another paper found that “cell cultures from various origins, chickens, dogs, ducks, guinea pigs, hamsters, horses, man, rabbits, rats, monkeys and swine have all been found to yield viruses spontaneously.” This means without adding any sample of body fluids, these cell cultures have or develop “viruses” as seen under the microscope. It’s more like break down material of cells in cell cultures that are looked at and interpreted as viruses.
He then presents an answer someone elicited from ChatGPT about the isolation of the polio virus and ChatGPT states that polio virus was never isolated directly from humans as per FOIA request. Injecting spinal tissue from so called polio victims into monkeys can cause illness. No controls were carried out, e.g. using spinal tissue of healthy people and injecting it into monkeys.

Image courtesy of Dr. Tom Cowan MD
5G and Covid Symptoms
I then looked into 5G/EMF effects on biological tissue and found a study3 showing that the symptoms of Covid can all be caused by 5G. The study primarily looked at the overlap of 5G exposure and Covid cases and found that areas with high 5G exposure had most of the Covid cases. The study states:
Statistical analysis showed that exposure to 5G mmW (which is present in combination with 1G-4G and other RFR sources like Wi-Fi) is a statistically significant factor associated with higher COVID-19 case and death rates in the U.S.

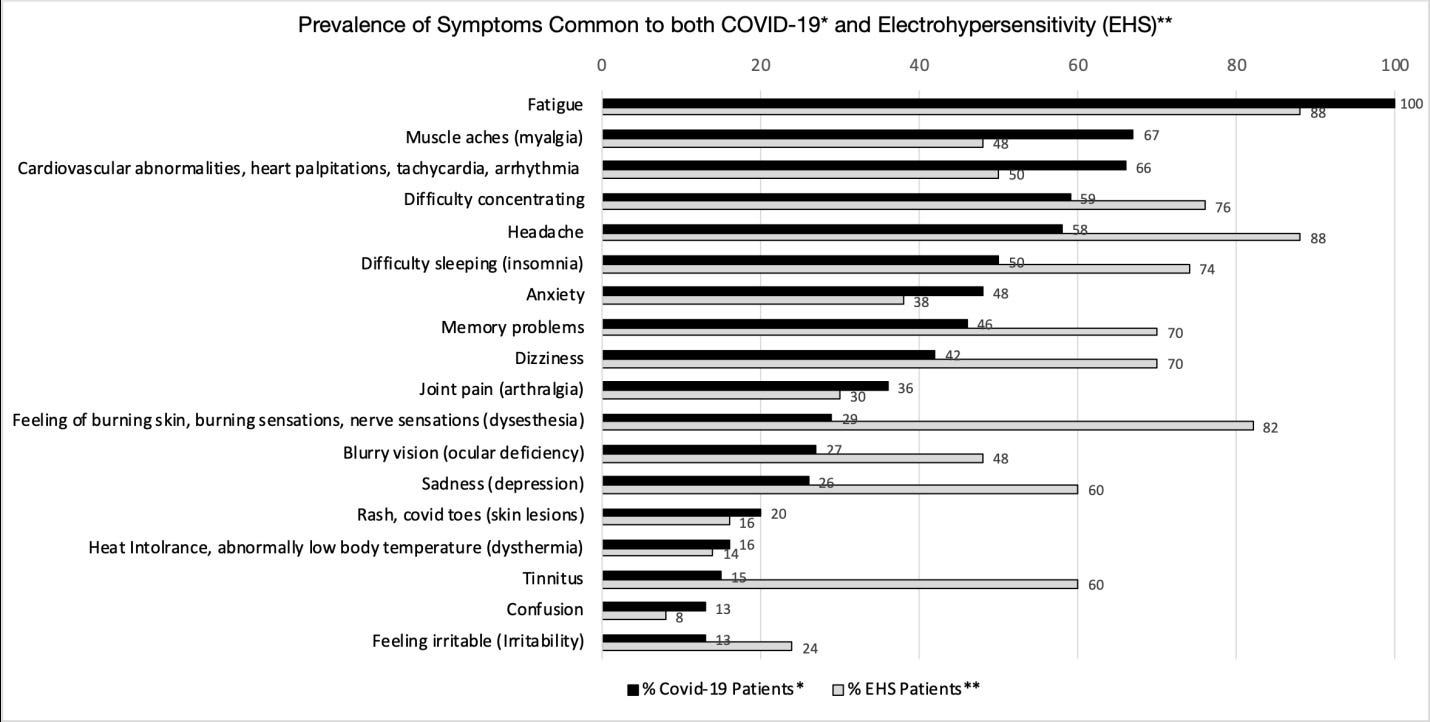
Some COVID-19 patients report they have been sick for many months, despite testing negative for the SARS-CoV-2 virus, with numerous symptoms of microwave sickness. Microwave sickness, which the World Health Organization refers to as idiopathic environmental intolerance attributable to electromagnetic fields (IEI-EMF), is the medical term for the syndrome of symptoms that result from chronic exposure to non-ionizing radiation. It is also referred to as electromagnetic sensitivity per the Americans with Disabilities Act (ADA) or electrohypersensitivity (EHS) in some scientific studies. However, electromagnetic illness (EMI) is perhaps a more appropriate term since RFR exposure has the potential to affect all humans and not only those who are highly sensitive to this radiation. Most of the symptoms that these long COVID-19 patients have in common with microwave sickness are headaches, fatigue, difficulty concentrating, memory problems, insomnia, cardiovascular abnormalities like palpitations and tachycardia, tinnitus, anxiety, depression, and skin lesions according to a COVID-19 Survey Report by Indiana University School of Medicine [21]. At least 24 of the long COVID symptoms reported in the survey are also symptoms of microwave sickness, aka EHS [22] (Figure 7).
They go on to explain how these radiofrequency waves can cause damage:
- Inflammation
- Oxidative stress
- Vitamin D receptor activity is lower
- deplete Glutathione, the body’s antioxidant
- change Hemoglobin structure reducing O2 uptake
- reduce mitochondrial function
- increase clotting as Vitamin D is an anticoagulant, but its function is inhibited due
to lower activity of Vitamin D receptors
- Rouleau formation of red blood cells, even red blood cell aggregation (clumping)
- alter cell membrane permeability and thus increases Calcium inside the cell which
has a host of unwanted effects.
- interfere with cell signaling and pulsed EMFs rapidly activate the mTOR signaling
pathway (more about mTor later)
Another study4 came to the same conclusion. EMF causes changes in blood and oxidative stress damaging tissues including endothelial cells (the inner lining of blood vessels) leading to local inflammation, patching up of the damage leading to occlusion of blood vessels. And it lowers the Immune system.
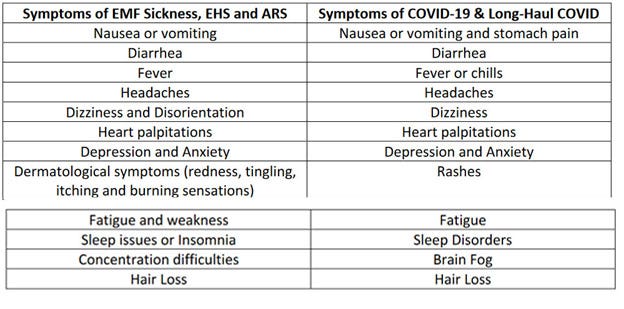
A paper called 5G, Epigenetics and Chronic Disease 4th Year Research Paper5 also shows the congruence of EMF sickness and Covid symptoms as the following table shows.
So now that we could establish that Covid symptoms, just like the Spanish flu over 100 years ago could be caused by EMF, let’s see if they can also cause Monkeypox symptoms.
What About Monkeypox?
The symptoms of Monkeypox as per this paper6, include fever, rash, sweats, chills, lymphadenopathy (swollen lymph nodes), headache, stiff neck, red eyes, runny nose, sore throat, cough, wheezing, shortness of breath, chest pain, nausea and/or vomiting, abdominal pain, myalgia, back pain, joint pain, confusion, and conjunctivitis. This sure sounds like flu like symptoms to me. What about the skin rash though? I’ll get into probable causes of that in while.
Now, what constitutes a Monkeypox case? The CDC website7 states:
Probable Case
No suspicion of other recent Orthopoxvirus exposure (e.g., Vaccinia virus in ACAM2000 vaccination) AND demonstration of the presence of
Orthopoxvirus DNA by polymerase chain reaction of a clinical specimen OR
Orthopoxvirus using immunohistochemical or electron microscopy testing methods OR
Demonstration of detectable levels of anti-orthopoxvirus IgM antibody during the period of 4 to 56 days after rash onset
Confirmed Case
Demonstration of the presence of monkeypox virus (MPXV) DNA by polymerase chain reaction testing or Next-Generation sequencing of a clinical specimen OR isolation of MPXV in culture from a clinical specimen
The main diagnostic criterium is a positive PCR Test. Everybody should know by now that the PCR method is not a test that can tell if anyone is sick. It’s humbug for the purpose of diagnosing anything. It’s a lab methodology to amplify DNA or RNA so scientists can play around with them.
The CDC further states:
The characteristic rash associated with mpox lesions involve the following: deep-seated and well-circumscribed lesions, often with central umbilication; and lesion progression through specific sequential stages—macules, papules, vesicles, pustules, and scabs.; this can sometimes be confused with other diseases that are more commonly encountered in clinical practice (e.g., secondary syphilis, herpes, and varicella zoster). Historically, sporadic accounts of patients co-infected with mpox virus and other infectious agents (e.g., varicella zoster, syphilis) have been reported, so patients with a characteristic rash should be considered for testing, even if other tests are positive. People with severe immunodeficiency (e.g., advanced HIV) may have skin lesions that are necrotic, diffuse, and plaque-like.
So, a case is a positive PCR Test done on people with skin lesions that can be easily confused with other causes such as Syphilis or in patients with other symptoms which can be a whole range of things.
Monkeypox Skin Lesions with Other Causes
I looked up other skin conditions that look like the pustules and blisters attributed to Monkeypox. There are a few papers discussing other skin conditions that can easily be confused with a Monkeypox rash. One paper8 states:
The differential diagnosis of widespread verrucous skin lesions in the Midwest and southern United States remains broad, including but not limited to disseminated Sporothrix schenckii, disseminated coccidioidomycosis, subacute progressive disseminated histoplasmosis, disseminated blastomycosis, cutaneous leishmaniasis, ecthyma gangrenosum, verrucous pyoderma gangrenosum (PG) and inflammatory pseudotumor associated with herpes simplex infection. PG, an inflammatory neutrophilic dermatosis, is an important differential diagnosis of verrucous lesions, particularly in regions of endemic mycosis. It is manifested by crusted and painful ulcers with irregular heaped borders and nonspecific histopathological features including neutrophilic infiltration, granuloma formation, necrosis and fibrosis.
Another study9 examined patients in the ER in a hospital in Marseille, France with skin lesions that looked like Monkeypox. They found that some patients had Syphilis, chickenpox, bacterial skin infection, gonococcus, herpes simplex and histoplasmosis.
Another paper10 I found lists the possible causes of generalized pustules as seen in Monkeypox cases.
Generalized pustules
Children
Erythema toxicum neonatorum
Transient neonatal pustular melanosis
Incontinentia pigmenti
Adults
IgA pemphigus foliaceus
Subcorneal pustular dermatosis
Impetigo herpetiformis
Acute generalized exanthematous
pustulosis
Eosinophilic pustular folliculitis
A paper11 on skin manifestations after ionizing radiation talks about Bullous Pemphigoid as a consequence of ionizing radiation. 5G and other telecommunication EMF is not ionizing radiation. But the mechanism is the activation of an auto-immune disease which can also be triggered by medications, infections, thermal or electrical burns, surgical procedures and trauma. Bullous Pemphigoid is characterized by subdermal blistering and in some cases could be confused with Monkeypox skin lesions.
Another paper12 lists a variety of other causes of skin lesions that can be interpreted as Monkeypox lesions:
Condition
Cutaneous manifestations
Smallpox: Initial macules become papules then vesicles and pustules; deep-seated, firm, umbilicated lesions Oropharyngeal lesions Prominent lymphadenopathy
Varicella: Simultaneous fever with pruritic rash; superficial papules and vesicles with irregular borders and centripetal distribution in various stages.
Genital herpes (herpes simplex virus; HSV): Grouped 2–4 mm vesicles with underlying erythema, progressing to vesiculopustules with erosions and ulcerations
Can have umbilicated appearance and be pruritic.
Measles: Initial development of Koplik spots prior to rash
Erythematous maculopapular lesions spreading cephalocaudally and centrifugally.
Hand, foot, and mouth disease: Uniform evolution of macules to papules then vesicles and pustules with predilection for palms, soles, and oropharynx.
Molluscum contagiosum: 2–5 mm pruritic, firm, dome-shaped shiny, centrally umbilicated lesions. Can have peripheral ‘crown’ of punctiform or radiating vessels.
Acute retroviral syndrome (human immunodeficiency virus; HIV): Diffuse, 5–10 mm, well-circumscribed pink-red macules and maculopapules. May be mildly pruritic.
Syphilis: Primary: Single genital papule evolving to a 1–2 cm painless ulceration with non-exudative base.
Secondary, early: diffuse, macular, flat, pale pink-to-brown elliptical lesions
Secondary, late: large, flattened papules or annular lesions
Disseminated gonococcal infection (DGI): Painless macules, papules, or petechiae evolving into pustules with central “gun-metal gray” necrotic areas and surrounding erythema.
Lymphogranuloma venereum (LGV): Isolated genital ulcer that heals with 2–6 week interval to development of large painful superficial or deep inguinal lymph nodes; may have rectal mass.
Chancroid: Erythematous genital papule evolving to pustule, followed by painful ulceration approximately 1–2 cm in diameter with yellow-gray exudate.
Meningococcemia: May initially present with nonspecific maculopapular rash for 1–2 days. Develop focal petechiae on trunk and legs; may involve oral mucosa; may coalesce into purpura and/or cutaneous hemorrhage and necrosis.
Staphylococcal scalded skin syndrome (SSSS): Erythema spreading to generalized body progressing to flaccid bullae with shallow erosions. Positive Nikolsky sign
No mucous membrane involvement.
Rocky Mountain spotted fever (RMSF): Blanching erythematous 1–4 mm macules evolving into petechiae beginning on distal extremities and spreading to trunk
May later involve palms and soles.
Toxic shock syndrome (TSS): Diffuse macular erythroderma
Mucous membranes may be involved with hyperemia. Desquamation 1–2 weeks after illness onset (often palms and soles).
Fungal infection: Cryptococcus: local cellulitis, ulceration, or whitlow at inoculation; umbilicated lesions with AIDS.
Histoplasmosis: varying papules, plaques, nodules, pustules, ulcers; lesions may resemble molluscum lesions.
Acute generalized exanthematous pustulosis (AGEP): Non-follicular pustules on edematous erythema. Starts on face and spread to trunk and limbs.
Erythema multiforme: Initial erythematous round papules with centripetal spread evolving to target lesions <3 cm in diameter with dusky central area, surrounded by ring of pale edema, and erythematous peripheral halo.
Pemphigus vulgaris: Primary lesions: tense, clear vesicles/bullae on head, trunk, mucosa which then become flaccid and turbid within several days, followed by rupture and areas of sensitive, denuded skin.
Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN): Coalescing erythematous macules with purpuric centers progressing to vesicles and bullae, followed by skin sloughing. Hemorrhagic mucosal erosions with white or gray membrane.
Sweet syndrome: Painful, edematous, red or violaceous papules, plaques, and nodules ranging in size up to several cm. Oral lesions may be present.
In the following image Dr. Tom Cowan narrowed down the skin diseases to what can be used to convince people that Monkeypox are real :
Pemphigoid, Pemphigus Vulgaris, Psoriasis, Exanthematous Pustulosis, Sweet Syndrome, Pityriasis lichenoides et varioliformis acuta. You can go to google and input these names and then go to Images and look at photos of these conditions. You will see, that they all look very similar.
In essence, skin only has so many ways it can react to something damaging, be it a bacterial infection, topical or systemic toxins such as pharmaceuticals, ionizing radiation or immunological issues. It can show a red rash, blisters, peeling, pustules and a few other reactions. Thus, skin issues often look very similar but are due to different causes.
The NIH put out a study listing other diseases that can cause skin issues that mimic monkey pox. As we have seen, the other Monkeypox symptoms are very unspecific such as fever, swelling of lymph nodes, headache, stiff neck, red eyes, runny nose, sore throat, cough, wheezing, shortness of breath, chest pain, nausea and/or vomiting, abdominal pain, myalgia, back pain, joint pain, confusion, and conjunctivitis. It could be anything and indicates a detoxing reaction just like flu symptoms, cold symptoms and “Covid symptoms”.
Can 5G/EMF cause skin reactions?
Yes, it can cause mostly rashes and burning. As we have seen earlier, EMF causes oxidative stress, inflammation, reduces Glutathione, changes the structure of hemoglobin reducing O2 uptake and reduce mitochondrial function and change cell membrane permeability. According to this paper14, they also activate the mTOR signaling pathway:
The stimulation of the mTOR cascade has been displayed to increase tumor growth through the regulation of glycolysis, angiogenesis, growth factor receptor pathway, lipid metabolism, and autophagy. mTor Dysregulation of this signaling pathway has been associated with the pathophysiology of cutaneous cancers [5], as well as immune-mediated dermatoses such as acne, psoriasis, vitiligo, and scleroderma. The PI3K-Akt-mTOR pathway plays a key role in cellular physiology, tissue homeostasis, and pathologic modification. Accordingly, alterations in normal homeostatic regulated pathways by mTOR can modulate protein synthesis to impact skin cell growth and proliferation, resulting in phenotypically diverse skin diseases including immune-mediated inflammatory dermatoses.
So, EMF not only can cause tumor growth in skin, but also activates acne, psoriasis and other skin conditions.
The paper5 I mentioned earlier also refers to Arthur Firstenberg’s book, The Invisible Rainbow, who describes that DNA is an antenna as are sweat glands. High powered and close up millimeter waves can cause burns on skin, but I couldn’t find any studies showing that 5G from towers cause skin lesions that look like what is attributed to monkeypox. However, since the rollout of the Covid jabs we have to factor in the presence of Graphene Oxide in the skin. A paper15 of 2010 states:
“This result confirms graphene oxide has high potential for transmitting signals at gigahertz ranges.” And: “If the body contained graphene oxide nano-particles then the fractal antennae nature of DNA would have transmitting capabilities and therefore be able to transmit 5G signals instead of just absorbing them into standing waves with no movement or momentum.”
As we have seen, 5G causes oxidative stress also in skin cells. This means reactive oxygen species ROS is causing damage in skin cells. If the detoxification and antioxidant defense system of the skin is overwhelmed, damage can occur. Since we also saw that 5G reduces the amount of Glutathione, the antioxidant defense system, damage is highly likely.
We now have to consider that Starlink and other satellite systems are not only able to put out 5G but other forms of high frequency energy waves. How is it that trees need to be cut down and many more 5G emitters need to be installed because the reach of 5G is much shorter than 4G but it can be beamed down from satellites in orbit at a much greater distance? We know that there are secret technologies that are decades ahead of what the public is allowed to know about. If mass outbreaks with skin lesions do happen, we must question what exactly is being emitted from these satellites and earth-bound emitters such as 6G,7G, Tesla energy (?) and what are the effects on our bodies in combination with toxic metals and Graphene Oxide.
Summary
In summary, Covid symptoms can be caused by 5G. Systemic Monkeypox symptoms can be caused by 5G. The combination of 5G/ other Gs with Graphene Oxide could also cause skin lesions. In addition, skin lesions attributed to Monkeypox can be a wide number of other things. The diagnosis of Monkeypox is based on a useless PCR test and skin lesions. Furthermore, the Monkeypox virus has never been isolated. In conclusion, Monkeypox does not exist. It’s a misdiagnosis and a conglomeration of symptoms that the media and WHO are cobbling together to scare the shit out the population to further their agenda of total global control with draconian measures from lockdowns, mask mandates and most of all forced injections to kill many of us and turn the rest into zombies hooked up to a hive mind.
Visit my book shop: www.anitabaxasmd.com
Note: The bananas in the monkey picture at the beginning are growing in my yard.
Sources:
3. COVID-19 Attributed Cases and Deaths are Statistically Higher in States and Counties with 5th Generation Millimeter Wave Wireless Telecommunications in the United States.
https://esmed.org/MRA/mra/article/view/2371
4. Evidence for a connection between coronavirus disease-19 and exposure to radiofrequency radiation from wireless communications including 5G Beverly Rubik 1 , 2 , * and Robert R. Brown 3
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8580522/
J Clin Transl Res. 2021 Oct 26; 7(5): 666–681. Published online 2021 Sep 29. PMCID: PMC8580522
5. https://naturopathicinstitute.org/wp-content/uploads/2022/08/Compiled-4th-Year-Research-Paper.pdf:
-CN, Submitted By: Charis Calender-Suemnick, NHP August 2022
6. https://academic.oup.com/cid/article/41/12/1742/344953
7. https://www.cdc.gov/poxvirus/mpox/clinicians/case-definition.html
8. https://link.springer.com/article/10.1186/s12879-023-08852-2
9. Journal of Medical Virology, How to distinguish mpox from its mimickers: An observational retrospective cohort study Coline Mortier, Hervé Tissot-Dupont, Florian Cardona, Christiane Bruel, Salima Lahouel, Hanane Lasri, Karim Bendamardji, Céline Boschi, Philippe Parola, Matthieu Million, Philippe Colson, First published: 06 October 2023 https://doi.org/10.1002/jmv.29147
https://onlinelibrary.wiley.com/doi/abs/10.1002/jmv.29147
10. https://link.springer.com/chapter/10.1007/978-3-642-97931-6_16#Tab1: non infectious pustules
11. Skin Manifestations after Ionizing Radiation Exposure: A Systematic Review by Luigi Bennardo 1,*,
Maria Passante, Bioengineering 2021, 8(11), 153; https://doi.org/10.3390/bioengineering8110153
12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9812851/
13. Viruses. 2023 Jul; 15(7): 1423. Published online 2023 Jun 23. doi: 10.3390/v15071423 PMCID: PMC10384785 PMID: 37515110
The Impact of COVID-19 Vaccination on Inflammatory Skin Disorders and Other Cutaneous Diseases: A Review of the Published Literature
Fabrizio Martora,* Teresa Battista, Angelo Ruggiero, Massimiliano Scalvenzi, Alessia Villani, Matteo Megna, and Luca Potestio
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10384785/
14. https://www.mdpi.com/2073-4409/12/12/1671: The PI3K-Akt-mTOR and Associated Signaling Pathways as Molecular Drivers of Immune-Mediated Inflammatory Skin Diseases: Update on Therapeutic Strategy Using Natural and Synthetic Compounds
Cells 2023, 12(12), 1671; https://doi.org/10.3390/cells12121671
15. 6. Kim et al. “Radio-frequency characteristics of graphene oxide.” Volume 97, Issue 19, Applied Physics Letters (AIP), 9 Nov. 2010, https://doi.org/10.1063/1.3506468
I totally agree. If microwaves already cause this damage, imagine how much more damage will be caused by introducing graphene oxide into the body. Graphene will act as a capacitor absorbing all this microwave energy causing more oxidative stress and therefore more damage.
Hi Anita,
A great summary and packaged nicely. Also good to see the real virology people credited.
I would add to potential graphene - morgellons fibres and bio film when it comes to skin issues today.
Also we are told its only non ionising radiation. Its hard to verify this as we can only read up to about 10 g but they have way higher capacity from the towers , <60g?.
I saw some early videos where people were using old Geiger counters and getting high readings in cities. That's probably why we need to buy old analogue giegers to know for sure.
Also I have been told that very high non ionising can do a lot of damage too
Regards, Matt